![]()
Before and After Photos of Various Cleft Types
These cases will show that surgical procedures must be done in “stages”. That is: a) The use of a removable plastic appliance, soon after birth, may or may not be necessary, b) Lip surgery – one or more procedures within the first year, c) Palatal surgery to close the palatal cleft generally between 18 to 24 months but sometimes later, d) Some orthodontics may be necessary in the deciduous dentition, mixed dentition and in the adult dentition.
Speech treatment will also include speech therapy and possibly some additional surgery.
These cases will clearly show that the best long term results will occur when treatment is performed in stages and the timing and type of surgery will vary according to the patient’s facial growth patterns. What is important is how the child looks and speaks when starting school and not how the child looks the first year of life.
Case #1: Cleft of Lip and Alveolus – No Palatal Cleft

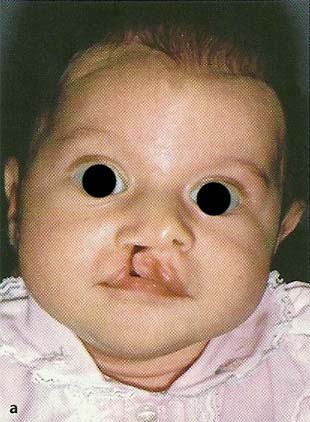
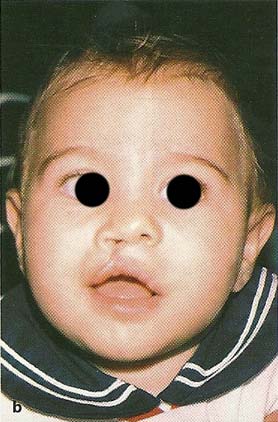
Case #2: Complete Unilateral Cleft Lip and Palate
Excellent facial aesthetics, dental occlusion and speech are possible. In most cases the palatal cleft would have to be closed between 18 to 24 months, sometimes even later depending on the size of the cleft space. With increased palatal growth, the palatal cleft becomes gradually smaller to permit better surgery which will lead to normal facial development and speech.
Case #3: Incomplete Bilateral Cleft Lip and Palate
This case demonstrates excellent facial growth changes in an incomplete bilateral cleft lip and palate treated conservatively with no presurgical orthopedics. Secondary alveolar bone grafts were placed in the cleft alveolus at 9 years of age.


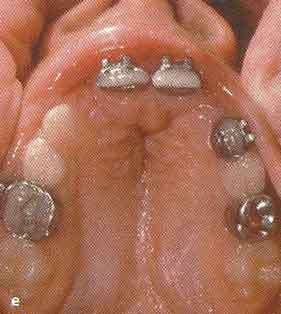
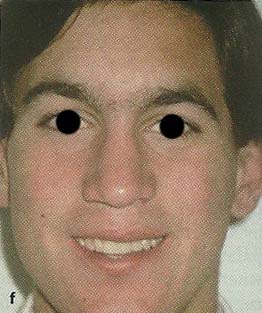
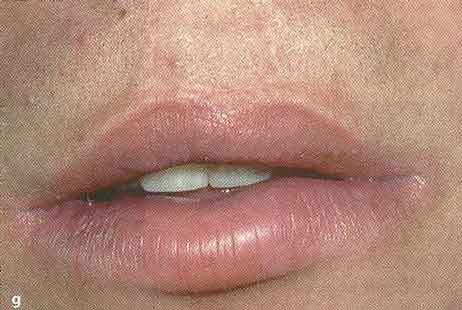

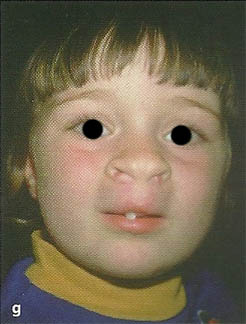
 a. Newborn. b. at 7 months, after lip closure. c. 4 years, 2 months. Note buccal crossbite on the left side. The crossbite was corrected by 4 years, 7 months using a fixed palatal expander. d. At 8 years after the central incisors were aligned and a secondary alveolar bone graft was performed. Note that lateral incisors are erupting through the graft. e. Palatal view at 7 years. f. Full face at 17 years. g. Close-up of lip. h. Occlusion at 17 years after orthodontics. i. Palatal view showing good vault space with minimal scarring.
a. Newborn. b. at 7 months, after lip closure. c. 4 years, 2 months. Note buccal crossbite on the left side. The crossbite was corrected by 4 years, 7 months using a fixed palatal expander. d. At 8 years after the central incisors were aligned and a secondary alveolar bone graft was performed. Note that lateral incisors are erupting through the graft. e. Palatal view at 7 years. f. Full face at 17 years. g. Close-up of lip. h. Occlusion at 17 years after orthodontics. i. Palatal view showing good vault space with minimal scarring.
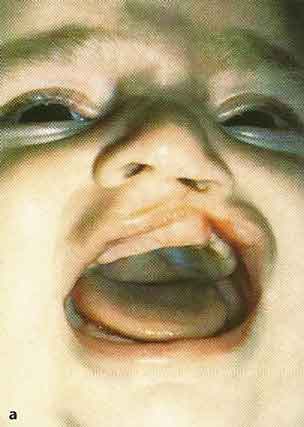
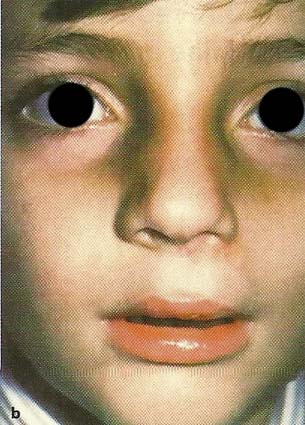
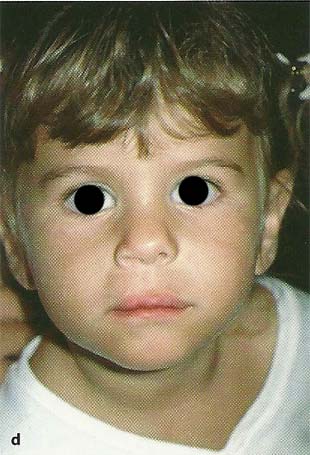
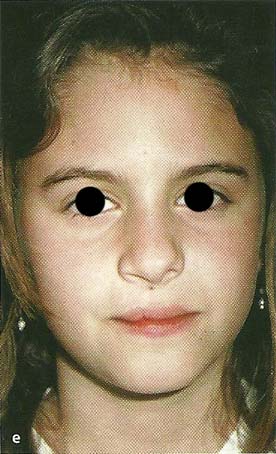
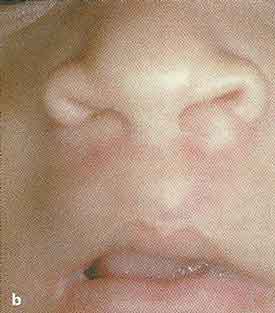
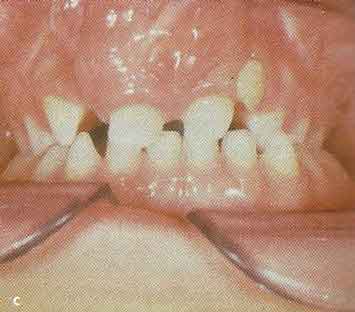
Case #4: Complete Bilateral Cleft Lip and Palate (CBCLP)
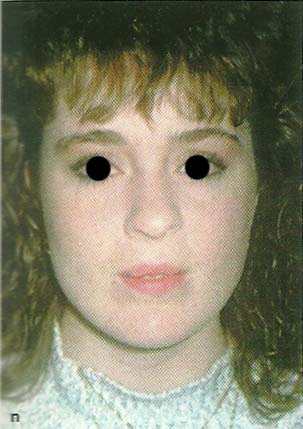
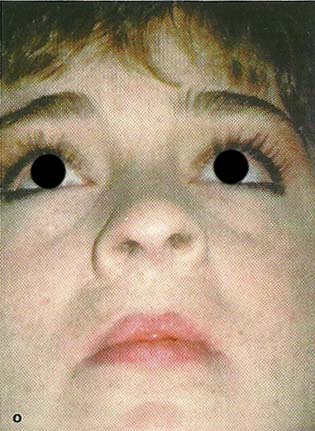
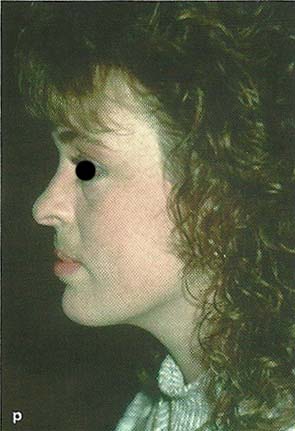
a. and b. At birth. An extremely protruding premaxilla. c. Head bonnet with elastic over the premaxilla. e. Occlusal view at 5 years of age. Note that the premaxilla is still protrusive. g. and h. The face at 5 years showing upper lip protrusion. i. At 11 years, 1 month, the premaxilla is still protruding. j. and k. Minor imperfections in the anterior teeth were corrected by the use of dental composite material. m. Ideal form with a normal palatal vault space. Good alveolar bone support to the lateral incisors. n., o., and p. Facial photographs at 20 years of age showing a harmonious and pleasing soft tissue profile. The most important part of treatment is to look to the future and be patient about how the face looks at a young age.
Serial photographs demonstrate excellent facial and palatal growth. No presurgical orthopedics other than the use of external elastics off a head bonnet for 10 days prior to lip surgery; arm restraints were used to prevent removal of the head bonnet. The palatal cleft was closed at 3 years of age. Secondary alveolar bone grafting was done at 8 years of age. A presurgical orthopedic appliance can be used soon after birth just to ventroflex the protruding premaxilla but not to bring it within the arch at this early age. Additional facial growth will gradually flatten the facial profile.










| < Previous (What Every Parent Should Know) | Next (Feeding Your Child) > |